
Page 7 - TBRA_Intake
P. 7
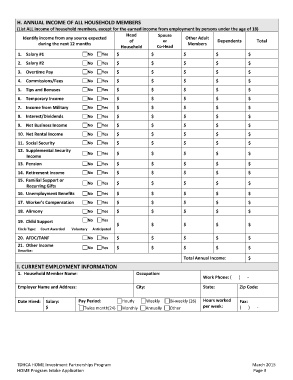
H. ANNUAL INCOME OF ALL HOUSEHOLD MEMBERS
(List ALL income of household members, except for the earned income from employment by persons under the age of 18)
Identify income from any source expected Head Spouse Other Adult Dependents Total
during the next 12 months of or Members
Household Co‐Head
1. Salary #1 No Yes $ $ $ $ $
2. Salary #2 No Yes $ $ $ $ $
3. Overtime Pay No Yes $ $ $ $ $
4. Commissions/Fees No Yes $ $ $ $ $
5. Tips and Bonuses No Yes $ $ $ $ $
6. Temporary Income No Yes $ $ $ $ $
7. Income from Military No Yes $ $ $ $ $
8. Interest/Dividends No Yes $ $ $ $ $
9. Net Business Income No Yes $ $ $ $ $
10. Net Rental Income No Yes $ $ $ $ $
11. Social Security No Yes $ $ $ $ $
No Yes $ $ $ $ $
12. Supplemental Security No Yes $ $ $ $ $
Income
13. Pension
14. Retirement Income No Yes $ $ $ $ $
No Yes $ $ $ $ $
15. Familial Support or No Yes $ $ $ $ $
Recurring Gifts
16. Unemployment Benefits
17. Worker’s Compensation No Yes $ $ $ $ $
18. Alimony No Yes $ $ $ $ $
19. Child Support No Yes $ $ $ $
$
Circle Type: Court Awarded Voluntary Anticipated
20. AFDC/TANF No Yes $ $ $ $ $
No Yes $ $ $
21. Other Income $ $ $
Describe:
Total Annual Income:
I. CURRENT EMPLOYMENT INFORMATION Occupation: Work Phone: ( ) ‐
1. Household Member Name:
Employer Name and Address: City: State: Zip Code:
Date Hired: Salary: Pay Period: Hourly Weekly Bi‐weekly (26) Hours worked Fax:
Other per week: ( ) ‐
$ {}
Twice month(24) Monthly Annually
TDHCA HOME Investment Partnerships Program March 2015
HOME Program Intake Application Page 3 