
Page 5 - TBRA_Intake
P. 5
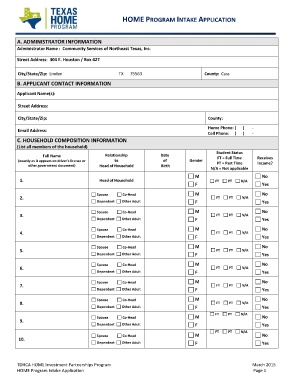
HOME PROGRAM INTAKE APPLICATION
A. ADMINISTRATOR INFORMATION
Administrator Name : Community Services of Northeast Texas, Inc.
Street Address: 304 E. Houston / Box 427
City/State/Zip: Linden TX 75563 County: Cass
B. APPLICANT CONTACT INFORMATION
Applicant Name(s):
Street Address:
City/State/Zip: County:
Home Phone: ( ) ‐
Email Address:
Cell Phone: ( ) ‐
C. HOUSEHOLD COMPOSITION INFORMATION
(List all members of the household)
Full Name Relationship Date Gender Student Status Receives
of FT = Full Time Income?
(exactly as it appears on driver’s license or to M PT = Part Time
other government document) Birth F N/A = Not applicable No
Head of Household M Yes
F FT PT N/A No
1. Head of Household M Yes
F FT PT N/A No
2. Spouse Co‐Head M Yes
3. Dependent Other Adult F FT PT N/A No
4. M Yes
5. Spouse Co‐Head F FT PT N/A No
6. Dependent Other Adult M Yes
7. F FT PT N/A No
8. Spouse Co‐Head M Yes
9. Dependent Other Adult F FT PT N/A No
10. M Yes
Spouse Co‐Head F FT PT N/A No
Dependent Other Adult M Yes
F FT PT N/A No
Spouse Co‐Head FT PT N/A Yes
Dependent Other Adult M
F FT PT N/A No
Spouse Co‐Head Yes
Dependent Other Adult
Spouse Co‐Head
Dependent Other Adult
Spouse Co‐Head
Dependent Other Adult
Spouse Co‐Head
Dependent Other Adult
TDHCA HOME Investment Partnerships Program March 2015
HOME Program Intake Application Page 1 